Nobel physics prize: First Nobel for climate science
Context:
The Nobel Prize for physics has been awarded to scientists from Japan, Germany and Italy for their work related to climate change.
Relevance:
Prelims, GS-III: Environment and Ecology, GS-III: Science and Technology
Dimensions of the Article:
- About the Nobel Physics Prize for Climate related work
- Details about the work of Nobel laureates
About the Nobel Physics Prize for Climate related work
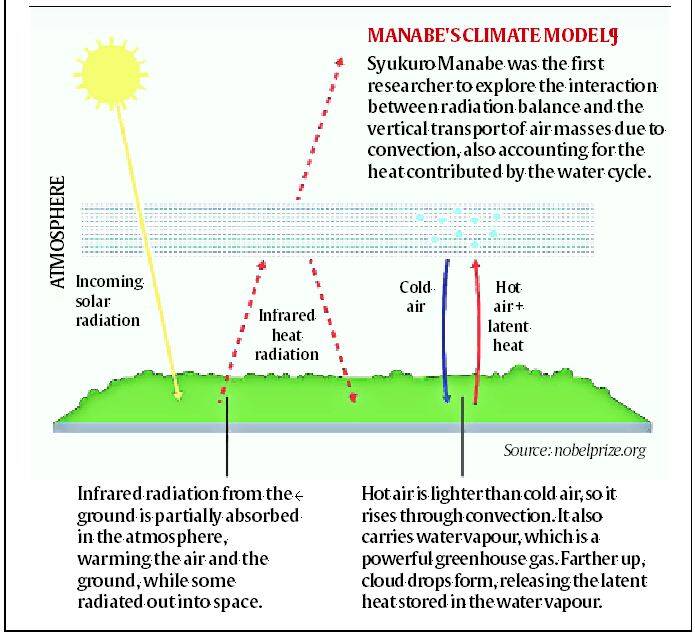
- One half of the Nobel Prize for physics has been awarded to Syukuro Manabe (90) and Klaus Hasselmann (89) – for their work in “the physical modeling of Earth’s climate, quantifying variability and reliably predicting global warming”.
- The second half of the prize was awarded to Giorgio Parisi (73) for “the discovery of the interplay of disorder and fluctuations in physical systems from atomic to planetary scales.”
- This is the first time climate scientists have been awarded the Physics Nobel.
- The IPCC had won the Peace Nobel in 2007, an acknowledgement of its efforts in creating awareness for the fight against climate change.
- The Chemistry Nobel was awarded to Paul Crutzen in 1995, for his work on the ozone layer – this is considered the only other time someone from atmospheric sciences has won this honour.
Details about the work of Nobel laureates
- A research paper by Syukuro Manabe and Richard Wetherald in 1967 had – for the first time described the impact of carbon dioxide and water vapour on global warming. It was the first description of the processes of global warming.
- Manabe and Wetherland also created a climate model for the first time. The sophisticated models that we run today, which are so crucial to climate science, trace their ancestry to that model created by Manabe.
- Manabe was also instrumental in developing the first coupled model, in which ocean and atmospheric interactions are modelled together, in the 1970s.
- Hasselmann is an oceanographer who is best known for his work on identifying specific signatures (“fingerprints” as the Nobel committee called them) in the climate phenomena that enabled scientists to ascertain whether these were caused by natural processes or human activities.
- Hasselmann enabled the field of attribution science. In the 1990s, and even in the early 2000s, there was a lot of debate over the cause of global warming – whether these were being driven by human activities, or were part of natural variability. Even the scientific world was divided. Hasselmann’s work on identifying these fingerprints has all but closed that debate now.
- Both Manabe and Hasselmann contributed to the first and third assessment reports of the IPCC while Hasselmann was an author in the second assessment report of IPCC as well.
- Georgio Parisi’s work was in advancing the understanding of complex systems – which are systems with a very high degree of randomness (weather and climate phenomena are examples of complex systems).
-Source: The Hindu
Health benefit package under AB PM-JAY revised
Context:
The Health Benefit Package (HBP) Master under the Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (AB PM-JAY) scheme has been revised.
Relevance:
GS-II: Social Justice and Governance (Issues related to Health, Welfare Schemes, Government Policies and Initiatives)
Dimensions of the Article:
- About Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (AB-PMJAY)
- Revised Health Benefit Package (HBP 2.2)
- About the National Health Authority (NHA)
About Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (AB-PMJAY)
- Ayushman Bharat – Pradhan Mantri Jan Arogya Yojana (AB-PMJAY) is a Centrally Sponsored Scheme having central sector component under Ayushman Bharat Mission anchored in the Ministry of Health and Family Welfare (MoHFW).
- It is an umbrella of two major health initiatives, namely Health and wellness Centres and National Health Protection Scheme.
- The PM Jan Arogya Yojana beneficiaries get an e-card that can be used to avail services at an empanelled hospital, public or private, anywhere in the country, with which they can walk into a hospital and obtain cashless treatment.
- The scheme has certain pre-conditions by which it picks who can avail of the health cover benefit. While in the rural areas the list is mostly categorized on lack of housing, meagre income and other deprivations, the urban list of PMJAY beneficiaries is drawn up on the basis of occupation.
- AB PM-JAY is the flagship scheme of the Union government as a part of the Indian government’s National Health Policy.
National Health Protection Mission (AB-PMJAY)
- AB-PMJAY provides a defined insurance benefit cover of Rs. 5 lakh per family per year. This cover will take care of almost all secondary care and most of tertiary care procedures.
- To ensure that nobody is left out (especially women, children and elderly) there will be no cap on family size and age in the scheme.
- The beneficiaries can avail benefits in both public and empanelled private facilities. All public hospitals in the States implementing AB-PMJAY, will be deemed empanelled for the Scheme.
- Benefits of the scheme are portable across the country and a beneficiary covered under the scheme will be allowed to take cashless benefits from any public/private empanelled hospitals across the country.
- To control costs, the payments for treatment will be done on package rate (to be defined by the Government in advance) basis.
Health and Wellness Centres (AB-PMJAY)
- Under this 1.5 lakh existing sub centres will bring health care system closer to the homes of people in the form of Health and wellness centres.
- These centres will provide comprehensive health care, including for non-communicable diseases and maternal and child health services.
Revised Health Benefit Package (HBP 2.2)
- Rates of some packages have been increased by 20 per cent to 400 per cent under the PM-JAY. Regular rates of the packages were being revised to provide better healthcare services.
- Rates of around 400 procedures have been revised and one new additional medical management package related to black fungus has also been added.
- The rate revision has been done in the following categories:
- radiation oncology procedures
- Medical Management procedures like procedure for dengue, acute febrile illness etc
- surgical package treatment for black fungus
- other procedures like Right/left heart catheterization, PDA closure, Arthrodesis, Cholecystectomy, appendicectomy etc.
- Under medical management procedures, rates for ICU with ventilator support have been revised by 100 per cent, rates for ICU without ventilator by 136 per cent.
- New packages are added to cover more disease conditions.
- HBP 2.2 packages for oncology will enhance cancer care for the beneficiaries in the country.
- The rationalised HBP will further improve the uptake of schemes in private hospitals leading to reduced out-of-pocket expenditure for the beneficiaries.
- Currently, Ayushman Bharat PM-JAY covers 1,669 treatment procedures out of which 1,080 are surgical, 588 medical and one unspecified package.
About the National Health Authority (NHA)
- National Health Authority (NHA) is the apex body responsible for implementing India’s flagship public health insurance/assurance scheme called “Ayushman Bharat Pradhan Mantri Jan Arogya Yojana”.
- The NHA been entrusted with the role of designing strategy, building technological infrastructure and implementation of “Ayushman Bharat Digital Mission” to create a National Digital Health Eco-system.
- National Health Authority (2019) is the successor of the National Health Agency, which was functioning as a registered society since 2018 (Not a Statutory body).
- NHA has been set-up to implement PM-JAY, as it is popularly known, at the national level.
- NHA is an attached office of the Ministry of Health and Family Welfare with full functional autonomy.
- NHA is also leading the implementation for Ayushman Bharat Digital Mission ABDM in coordination with different ministries/departments of the Government of India, State Governments, and private sector/civil society organizations.
- NHA is governed by a Governing Board chaired by the Union Minister for Health and Family Welfare and it is headed by a Chief Executive Officer (CEO), an officer of the rank of Secretary to the Government of India, who manages its affairs.
-Source: The Hindu
SC on NEET-SS: Medical education has become a business
Context:
The Supreme Court said the tragedy of medical education in the country was that it had become a business – while examining the National Eligibility-cum- Entrance Test- Super Specialty (NEET-SS) 2021.
Relevance:
GS-II: Social Justice and Governance (Issues related to Education, Government Policies and Initiatives)
Dimensions of the Article:
- What the SC said on NEET-SS 2021 changes?
- Current situation of inadequacy in Healthcare workforce
- NITI Aayog’s proposal and issues with it
- Way Forward
What the SC said on NEET-SS 2021 changes?
- The Supreme Court pulled up the government and the National Board of Examinations (NBE) for making last-minute changes to the pattern of the National Eligibility-cum- Entrance Test- Super Specialty (NEET-SS) 2021.
- The court noted that questions under the revised pattern were wholly from General Medicine, which was a feeder category. The earlier pattern had 60% of the questions coming from the student’s chosen field of speciality and the rest from the feeder category.
- The court reasoned that this sudden change was meant to favour General Medicine, in which the largest pool of students were found, to fill the seats.
- The court surmised that private institutions benefited with the change in exam pattern. It remarked that since seats in government colleges never lay vacant, it must be for their private counterparts that the pattern was altered.
- On this change, the SC said that “medical education has become a business, and medical regulation has also become a business.”
Current situation of inadequacy in Healthcare workforce
- India’s availability of doctors per thousand population does come close to the World Health Organisation’s prescribed doctor-patient ratio of 1:1000 if we include all the registered allopathic, homeopathic, ayurvedic and unani doctors. But the number of doctors who practise is much lower.
- It is also far lower than many countries including Russia, the USA, and all the European Union countries where the ratio is above 3 doctors per one thousand population. Unless we increase the ratio to the level of better performing countries on the health front, poor people in India will continue to suffer.
- As a major impediment for achieving the health-related Sustainable Development Goals (SDG) there is a serious shortage of health workers, especially doctors, in some northern States.
- Health workers are critical not just for the functioning of health systems but also for the preparedness of health systems in preventing, detecting and responding to threats posed by diseases such as COVID-19.
- The doctor-population ratio in northern States is far short of the required norm, while the southern States, barring Telangana, have enough doctors in possession- hence, the healthcare workforce crisis has been aggravated by the imbalances within the country.
- The problem of shortage of doctors and other support staff has been allowed to linger for the past several decades due to short-sighted policies of the institutions such as Medical Council of India
Medical Education as the building block of Health system
- Medical education is the bedrock on which the needs of ‘human resources for health’, one of the major building blocks of any health system, are met.
- Today’s health professionals are required to have knowledge, skills, and professionalism to provide safe, effective, efficient, timely, and affordable care to people.
NITI Aayog’s proposal and issues with it
- NITI Aayog’s proposal for the taking over of district hospitals for converting them into teaching hospitals by private entities has reasons to be deeply concerned.
- The most important concern is that the private sector in medical education will be encouraged by the implementation of such a policy. Private players treat medical education as a business.
- It will also directly aid the corporatisation processes of healthcare provisioning while the under-resourced public health system will be a collateral damage.
- District hospitals are considered as the last resort for the poor.
- The corporatisation will make the services very costly and exclude them from getting care.
- Even from the perspective of producing more doctors to meet the shortages in under-served areas, this is unlikely to yield the desired result.
- Additionally, the medical graduates trained in such private sector ‘managed’ medical colleges will prefer to find employment in corporate hospitals and not in rural areas to regain their investment.
- Further, this proposal is not aligned with India’s national health policy goals like achieving universal health care and health equity. Instead, it will widen health inequalities further.
Way Forward
- The 500+ medical colleges in India have only over 75,000 seats for the MBBS course and only half these seats are in state-run medical colleges. If India has to achieve the doctor-patient ratio of 1:1,000, we need nearly 20 lakh more doctors by the year 2030.
- Time has come that we reform the medical education system, end the pervasive corruption in these regulatory institutions and ensure that we carry out the expansion in such a way that we produce the required number of doctors to look after our population.
- Today’s medical education should be able to groom such professionals to face medicine of the 21st century. The Lancet report, ‘Health Professionals for a new century: transforming health education to strengthen health systems in an interdependent world’ (2010) outlines key recommendations, to transform health professional education, needs to be looked upon.
- Extending teaching privileges to practising physicians and allowing e-learning tools will address the shortage of quality teachers across the system. Together, these reforms could double the existing medical seats without compromising on the quality of teaching.
- There should be a substantial step-up in public investment in medical education.
- By establishing new medical colleges, the government can increase student intake as well as enhance equitable access to medical education.
- Besides, it must allocate adequate financial resources to strengthen the overall capacity of existing medical colleges to enrich student learning and improve output.
-Source: The Hindu
India on protecting the Antarctic and designating MPAs
Context:
India has extended support for protecting the Antarctic environment and for co-sponsoring the proposal of the European Union for designating East Antarctica and the Weddell Sea as Marine Protected Areas (MPAs) at a high-level ministerial meeting.
Relevance:
GS-III: Environment and Ecology (Environmental Pollution and Degradation, Conservation of Environment and Ecology, International Organizations/Treaties and Conventions)
Dimensions of the Article:
- About India’s statements regarding Protection of Antarctica
- What are Marine Protected Areas (MPAs)?
- Commission for the Conservation of Antarctic Marine Living Resources (CCAMLR)
- India’s programmes in Antarctica
About India’s statements regarding Protection of Antarctica
- India has extended support for co-sponsoring a proposal of the European Union for designating East Antarctica and the Weddell Sea as Marine Protected Areas (MPAs).
- India has said that the two proposed MPAs are essential to regulate illegal unreported and unregulated fishing.
- India’s Earth Sciences Minister urged the Commission for the Conservation of Antarctic Marine Living Resources (CCAMLR) member countries to ensure that India remains associated with the formulation, adaptation and implementation mechanisms of Marine Protected Areas (MPAs) in future.
What are Marine Protected Areas (MPAs)?
- Marine Protected Areas (MPAs) are marine protected areas that provides protection for all or part of its natural resources.
- It involves the protective management of natural areas according to predefined management objectives.
- MPAs can be conserved for a number of reasons including economic resources, biodiversity conservation, and species protection.
- They are created by delineating zones with permitted and non-permitted uses within that zone.
- It offers nature-based solutions to support global efforts towards climate change adaptation and mitigation
Issues with MPAs
- Most existing MPAs do not have enough human and financial resources to properly implement conservation and management measures.
- Lack of strictly and permanently protected MPAs limits our ability to support climate change adaptation and mitigation.
Significance of declaring MPAs
- Strictly protected MPA networks in coastal carbon habitats (mangroves, seagrasses, salt marshes) can ensure that no new emissions arise from the loss and degradation of these areas. At the same time, they stimulate new carbon sequestration through the restoration of degraded coastal habitats.
- Well-integrated MPA networks can increase species survival by allowing them to move around and escape certain pressures.
- In addition, MPAs where stressors are controlled can be used as sentinel (research) sites to help track the effects of climate change.
Commission for the Conservation of Antarctic Marine Living Resources (CCAMLR)
- CCAMLR was established by international convention in 1982 with the objective of conserving Antarctic marine life. This was in response to increasing commercial interest in Antarctic krill resources, a keystone component of the Antarctic ecosystem and a history of over-exploitation of several other marine resources in the Southern Ocean.
- It is an international commission with 26 Members, and a further 10 countries have acceded to the Convention. Based on the best available scientific information, the Commission agrees on a set of conservation measures that determine the use of marine living resources in the Antarctic.
- India has been a permanent member of the CCAMLR since 1986. Work pertaining to the CCAMLR is coordinated in India by the Ministry of Earth Sciences through its attached office, the Centre for Marine Living Resources and Ecology (CMLRE) in Kochi, Kerala.
India’s programmes in Antarctica
- Indian Antarctic Programme: The Indian Antarctic Programme is a scientific research and exploration program under the National Centre for Antarctic and Ocean Research (NCPOR) that started in 1981 when the first Indian expedition to Antarctica was made.
- Dakshin Gangotri: Dakshin Gangotri was the first Indian scientific research base station established in Antarctica, as a part of the Indian Antarctic Program. However, now it has weakened and become just a supply base.
- Maitri: Maitri is India’s second permanent research station in Antarctica. It was built and finished in 1989 and is situated on the rocky mountainous region called Schirmacher Oasis.
- Bharti: Bharti, India’s latest research station operation since 2012. It has been constructed to help researchers work in safety despite the harsh weather and it is India’s first committed research facility and is located about 3000 km east of Maitri.
READ OTHER NEWS HERE: https://www.pmias.in/current-events/